- A hypertensive emergency is defined by target-organ damage, not the number alone; the Turkish Society of Cardiology specifies a situation in which blood pressure must be "lowered very urgently, by the parenteral route."
- The American Heart Association's 14 August 2025 update keeps the 180/120 mmHg threshold and writes the rule plainly: "Call 911 if your blood pressure is higher than 180/120 and you are experiencing symptoms."
- The Ministry of Health's 18.3% figure (population aged 15+) is a self-report/diagnosed-prevalence number; in direct-measurement field studies the real prevalence in Turkish adults is about 30% (PatenT2: 30.3%) — so most of the population lives undiagnosed. The Ministry diagnosed 278,000 new patients between July 2021 and March 2025.
- The Turkish Statistical Institute's 2024 mortality bulletin attributes 36% of all deaths to circulatory disease, with 42.9% of those from ischemic heart disease and 18.3% from cerebrovascular disease (this 18.3% death share is only a numerical coincidence with the prevalence figure above) — uncontrolled hypertension is the principal trigger of both.
- Do not give sublingual capsules (nifedipine), aspirin, or extra doses on scene; abrupt lowering precipitates stroke and ischemia. The two correct actions are to repeat the measurement and, if symptoms are present, to call 112.
Quick Answer: When a blood-pressure reading crosses 180/120 mmHg, only one decision matters in the next three seconds — are there warning symptoms? If chest pain, shortness of breath, severe headache, blurred vision, speech difficulty, sudden numbness, altered consciousness or vomiting is present — even one — call 112 immediately; if you prefer a specific private hospital, open a parallel call to Nova Ambulans. If the number is high but there are no symptoms, rest 30 minutes in quiet, remeasure on the same arm — if still ≥180/120, see your family physician or the emergency department the same day. The American Heart Association's (AHA) 14 August 2025 update calls this threshold "a medical emergency that needs minutes, not hours," and writes the rule word for word: "Call 911 if your blood pressure is higher than 180/120 and you are experiencing symptoms" [6]. The Turkish Statistical Institute's (Türkiye İstatistik Kurumu, TÜİK) bulletin of 19 June 2025 attributes 36% of all 489,361 deaths in Turkey in 2024 to circulatory-system diseases — uncontrolled hypertension is the earliest and most controllable link in that chain [2].
What a Hypertensive Crisis Is — and Why the Number Alone Isn't an Emergency
A hypertensive crisis is the situation a patient describes as "my blood pressure suddenly went up" — readings that abruptly cross the 180/120 mmHg threshold. Contrary to public perception, however, the number on its own is not enough to send someone to the emergency room; the decision is determined by whether blood pressure has begun to damage target organs — brain, heart, kidneys, retina and large vessels. The Turkish Society of Cardiology (TKD) defines a hypertensive emergency precisely: "situations in which blood pressure must be lowered very urgently, by the parenteral route, in order to prevent or limit target-organ damage" [3]. That sentence packs two points: the threshold is organ damage, and the treatment is intravenous — so it cannot be resolved at home.
The clinical literature reserves a separate label, a hypertensive urgency, for the same severity without target-organ damage. The same guideline describes urgency as a picture "in which lowering blood pressure over hours or days, generally with oral antihypertensives, is preferred" [3]. The practical translation: a reading of 195/118 with no complaint, which on remeasurement is still high, is an urgency, not an emergency, and is managed by a same-day outpatient or emergency-department visit. The same 195/118 reading accompanied by chest pain, vision loss or confusion needs 112 and intensive care.
Pace of rise matters as much as the absolute value. The European-led 2024 Malignant Hypertension review notes: "BP must be lowered within hours to mitigate patient risk. Both absolute BP levels and the pace of BP rise determine risk of target-organ damage" [8]. So a reading of 190/115 in a patient who has lived at 160/100 for years is different from — and less alarming than — the same number in someone whose blood pressure has never been high.
Emergency or Urgency? Target-Organ Damage Decides
The rule is simple: a high number plus signs that one or more target organs are involved equals a hypertensive emergency. The organ-symptom mapping below not only guides the bystander on scene, it also tells you which symptoms to relay when you call 112. Reminder: in Turkey, stroke symptoms and the FAST test often appear as a standalone topic, but most cases trace back to untreated hypertension.
- Brain — severe, "worst-ever" headache; unilateral weakness; facial asymmetry; speech difficulty; sudden vision loss or double vision; altered consciousness; seizure; sudden balance loss. The list overlaps the picture of ischemic or hemorrhagic stroke; hypertensive crisis and stroke are clinically intertwined.
- Heart — chest pain or pressure, dyspnea, exertional chest tightness, pain radiating to the arm or jaw, tearing pain to the back (suspect aortic dissection). The Turkish Society of Cardiology guideline calls out this combination: "A patient with aortic dissection whose blood pressure is >160/110 mmHg belongs in the hypertensive-emergency group" [3].
- Lungs — resting dyspnea, breath shortness on lying flat, pink frothy sputum, rapid weight gain and leg edema (acute left heart failure).
- Kidneys — markedly reduced urine output over the last 12 hours, hematuria or foamy urine, rapidly developing hand-and-foot swelling.
- Eyes — sudden blurred vision, curtain-like vision loss, eye burning or scotomas (signs of papilloedema or retinal hemorrhage).
- Vessels — tearing back pain, unilateral pulse loss, a cold finger, sudden severe abdominal pain.
If any one symptom is present, drop the "let's wait, maybe it passes" line. The 2024 Journal of the American College of Cardiology review names "non-adherence to the antihypertensive regimen" as the most common cause of malignant hypertension [8]; in other words, most crises are missed medication coming home, and the right answer is not to add another dose at home but to move the patient to a place where blood pressure can be lowered under monitoring.
A 5-Step Decision Tree: 112, Family Physician, or Home?
Bystanders need an executable flow, not a panicked guess. The five steps below blend the American Heart Association's 14 August 2025 update with the Turkish Society of Cardiology's parenteral-treatment criterion.
Step 1 — Measure correctly (do not decide before remeasuring)
Sit in a chair with back support, feet on the floor; no smoking/caffeine/exercise/meal in the last 30 minutes; rest silently for 5 minutes; the cuff on the upper arm at heart level, neither too tight nor loose. Measure once, wait 1–2 minutes, measure on the same arm again. The first reading is typically the higher one; use the second. Wrist cuffs alone are not reliable.
Step 2 — Read the number
Is the second reading 180/120 mmHg or higher? If no, this article isn't your situation; a scheduled family-medicine visit for medication review is enough. If yes, go to step 3.
Step 3 — Check for symptoms
Is any of the list present?
- Chest pain, shortness of breath, or sudden back pain
- Severe headache (especially sudden-onset "worst of my life")
- Blurred vision, double vision, or vision loss
- Slurred speech, word-finding difficulty, or confusion
- Unilateral weakness, facial asymmetry, or arm drift
- Altered consciousness, disorientation, or unusual drowsiness
- Seizure
- Vomiting (especially with headache)
- New leg edema or foamy urine
If yes, go to step 4; if no, go to step 5.
Step 4 — Symptom present: call 112 now
Put the phone on speaker. Prepare: address, patient's age, chronic medications (collect the boxes), last reading, and time it was taken. The 112 Command-and-Control Centre routes the call to the nearest hospital with the right intensive-care capacity. If you prefer a specific private hospital, place a parallel Nova Ambulans call — for Istanbul ambulance response patterns by district, hour and traffic, see How Long Does an Ambulance Take in Istanbul (2025). While waiting: lay the patient supine, head elevated 30–45 degrees, loosen collars and tight clothing, keep the room quiet; do not offer food or drink (especially coffee, cola, tea).
Step 5 — No symptoms: 30 minutes of controlled rest
The patient sits in a quiet room, lights dimmed, feet elevated, eyes closed for 30 minutes. The bystander keeps talk to a minimum and silences phones. Remeasure at the end. Two possible outcomes:
- Down to <180/110, still no symptoms: This is a hypertensive urgency settling; arrange a same-day or next-morning family-medicine visit; the regimen is inadequate.
- Still ≥180/120, no symptoms: Go to the emergency department in person. If the patient is elderly, pregnant, has Chronic Obstructive Pulmonary Disease (COPD)/asthma, chronic kidney disease or known cardiac disease, prefer 112 instead — in these subgroups, persistent high readings work against time.
On-Scene Dos and Don'ts
Keep the "do" list short — the real treatment of hypertensive crisis starts in hospital; on scene, the bystander's only job is to not make things worse.
Do:
- Collect every chronic-medication box the patient takes; write the last reading and its time on a note placed with the boxes for the crew.
- Elevate the head of the bed to 30–45 degrees; if vomiting, place in the recovery (lateral) position. Our step-by-step recovery position guide covers technique.
- Keep the cuff snug — fingertip-fit, not constrictive; alternate arms between consecutive measurements.
- Place 112 on speaker; relay onset time, symptom list and readings in sequence.
- Do not add an extra dose of the patient's known antihypertensive if that day's planned dose was already taken; if it was missed and the patient is awake and able to swallow, only give the planned dose with the dispatcher physician's phone-confirmed approval.
Don't:
- Do not give sublingual nifedipine (short-acting Adalat). The Turkish Society of Cardiology guideline recommends parenteral, in-hospital lowering for hypertensive emergencies [3]; sublingual administration has long been known to drop blood pressure within minutes and precipitate stroke.
- Do not offer an unknown herbal "blood-pressure lowerer" (vinegar water, garlic, lemon, ginkgo, etc.); effects are unpredictable and adverse-effect reporting is sparse.
- Aspirin is considered only when a classic heart-attack picture is present (chest pain, left-arm radiation, cold sweat) and the patient is conscious and able to swallow; in a stroke picture it raises bleeding risk — never give without telephonic approval from the 112 medical command.
- Do not drive the patient yourself — the ambulance team opens IV access en route, runs an ECG, and can deliver the first antihypertensive; a private car offers none of this.
- Avoid "calming" home remedies such as hot showers, cold showers or massage; a hot shower in particular causes peripheral vasodilation and impairs cerebral perfusion.
How to Measure Blood Pressure Correctly — Before You Diagnose a Crisis
A wrong measurement leads to a wrong decision. The four most common errors we see at the clinic — an undersized cuff, ignoring a left–right arm difference, smoking or coffee just before measuring, and placing the cuff over a sleeve — inflate the reading by 10–15 mmHg, and that single distortion can drive an unnecessary ambulance call. Correct technique is six items:
- Sit in a chair with back support; feet on the floor, legs uncrossed; rest silently for 5 minutes.
- No smoking, caffeine, physical exertion or meal in the last 30 minutes; empty your bladder beforehand.
- Use an upper-arm digital device on an international clinical validation list; the cuff bladder should encircle 80–100% of your upper-arm circumference.
- Place the cuff on the bare arm (not over a sleeve), at heart level, 2 cm above the antecubital fossa.
- Do not talk or interact with a phone during the reading; eyes forward.
- Wait 1–2 minutes between readings; take the second reading on the same arm. At first visit, also measure both arms and use the consistently higher arm as your reference.
For the first day, take morning and evening readings for seven consecutive days; that log is the single most valuable input a family physician has for tuning the regimen.
Hypertension in Turkey: Prevalence, Mortality and the Screening Programme
A national frame for the topic. The Ministry of Health's 17 May 2025 World Hypertension Day announcement reported that "between July 2021 and March 2025, 278,000 of the registered persons screened were diagnosed with hypertension," and that "a 2023 study found hypertension prevalence at 18.3% among Turkey's population aged 15 and over" [1]. That 18.3% is a self-report/diagnosed-prevalence figure (population aged 15+, largely based on self-report and recorded diagnoses); the directly measured prevalence in Turkish adults is far higher. The Turkish hypertension-prevalence study PatenT2 (2012, ages 18 and over) reports a measured prevalence of 30.3% [9]; TURDEP-II similarly found roughly 31%. In other words about one in three adults is hypertensive, and a large share remains undiagnosed — the 18.3% official figure reflects the rate of recorded diagnoses, not how widespread the disease actually is. The Disease Management Platform (Hastalık Yönetim Platformu, HYP) — Hypertension Module — running under family medicine is the operational instrument behind those numbers.
The mortality picture comes from the Turkish Statistical Institute's bulletin of 19 June 2025: "The number of deaths was 526,416 in 2023 and 489,361 in 2024"; when analysed by cause, "circulatory-system diseases ranked first at 36%," and within that class, "42.9% of deaths were due to ischemic heart disease, 23.9% to other heart diseases and 18.3% to cerebrovascular disease" [2]. Hypertension is the most important modifiable risk factor for both the ischemic heart and cerebrovascular paths; a meaningful share of those 489,361 deaths begins with a controllable blood-pressure history.
An international frame closes the picture. The World Health Organization's (WHO) hypertension fact sheet, last updated 25 September 2025, reports: "An estimated 1.4 billion adults aged 30–79 years worldwide had hypertension in 2024; this represents 33% of the population in this age range" [7]. Note that this measured 33% global figure is consistent with the Turkish adult field data cited above (PatenT2: 30.3%), whereas the 18.3% official figure looks lower because it was obtained with a different method (self-report/records) [9]. The World Health Organization's (WHO) standard definition is ≥140/90 mmHg, though treatment-initiation thresholds vary by guideline. The Turkish Hypertension Consensus Report 2025, published on 26 November 2025 with the signatures of seven professional societies (Turkish Society of Cardiology, Turkish Society of Internal Medicine, Turkish Society of Endocrinology and Metabolism, Turkish Society of Nephrology, Turkish Society of Hypertension and Renal Diseases, Turkish Society of Family Medicine Specialists, and the Academic Geriatrics Society), defines normal blood pressure as systolic <120 / diastolic <80 mmHg, sets the threshold for combination drug therapy at ≥140/90 mmHg, and — for the first time — adds a dedicated chapter on hypertensive emergencies [5]. This is the current reference your Turkish family physician now works to.
Special Populations: Elderly, Pregnant, Diabetic, Chronic Kidney Disease
The decision tree is the same; the thresholds shift in some groups.
Elderly (≥80 years). Rapid lowering disrupts cerebral perfusion and raises the risk of fall, syncope and ischemic stroke; medication-dose doubling at home is the most common error in this group. An 80-year-old reading 200/100 without symptoms is better served by a same-day emergency-department visit than by 112; but chest pain, shortness of breath, or severe headache shifts the picture back to immediate ambulance. For broader at-home monitoring, our home care and ambulance support for older adults guide covers medication scheduling and continuous oversight.
Pregnancy. The threshold drops. After the 20th gestational week, readings ≥140/90 mmHg paired with headache, vision change, upper-abdominal pain, edema, or reduced urine output define preeclampsia and sit at the doorstep of eclampsia (seizure); a reading of 150/95 is not "within the normal range" for a pregnant patient. Call 112 directly and report the gestational week; while waiting, place the patient in left-lateral decubitus to lift the gravid uterus off the great vessels and preserve maternal–fetal blood flow.
Diabetes. Target blood pressure is typically <130/80 mmHg; autonomic neuropathy often accompanies long-standing disease, which makes symptoms like dizziness or fatigue harder to interpret. Hypertensive-crisis and hypoglycemia presentations can overlap; if possible, check a fingerstick glucose at the same time. For the sugar side of the same scene, read our diabetes and emergencies guide.
Chronic kidney disease, and dialysis patients in particular, see hypertensive crises far more often than the general population; fluid shifts around dialysis can trigger sudden rises. On a dialysis day with sudden worsening, call your dialysis centre; but the 180/120 + symptom rule still holds — that combination still means 112.
The Istanbul Frame: 112, the Command-and-Control Centre, and Hospital Choice
In Istanbul, after the hypertensive-emergency decision the chain runs like this: the 112 Command-and-Control Centre classifies the symptom category on the call, dispatches the nearest appropriately-equipped ambulance, and coordinates the hospital handoff; a chest-pain-dominant case is routed to a cardiac-intensive-care–capable centre, a neurology-dominant case to a stroke centre authorised under the Turkish Ministry of Health's 18 July 2019 "Directive on Health Services for Acute Stroke Patients." As a bystander you do not need to know the address or the hospital name — 112 does the routing.
A parallel private-ambulance call — most useful when you prefer a particular private hospital or the patient's records sit at a specific institution — shortens your individual response time and preserves your insurance/hospital preference during transfer. For when each option fits, see Difference Between 112 and a Private Ambulance. For Istanbul response times by district, hour, and traffic, see our How Long Does an Ambulance Take in Istanbul (2025) analysis — the "five minutes saved" calculus is the difference for the brain, heart, and kidney in a 188/118 reading.
What Happens Next: The First 7 Days After Discharge
A discharge after a hypertensive crisis is as critical as the home decision at the start of this article. The point the 2024 Journal of the American College of Cardiology (JACC) review underlines is adherence: "Non-adherence to the antihypertensive regimen remains the most common cause for malignant hypertension" [8]. A practical 7-day checklist after discharge: 1) gather every new medication box in one place and set a phone alarm for each scheduled dose; 2) take a morning and evening home blood-pressure reading, log it; that record is the basis for your family physician's first dose adjustment; 3) gentle salt restriction (<5 g/day) and fluid balance — avoid the salty foods that swell the ankle; 4) severe headache, vision change, shortness of breath, or another reading above 180/120 still means 112 — "it happened once and passed" is not a closing chapter; 5) book the family-medicine appointment within seven days.
After discharge, especially for elderly or bedbound patients, our hospital-to-home discharge and transport planning guide is the right starting point for vehicle choice and home-setup checklists.
Frequently Asked Questions
My BP is 180/110 but I have no symptoms — should I call 112?
No — if there are no warning symptoms, the picture is not a hypertensive emergency but a hypertensive urgency. The Turkish Society of Cardiology defines this as a state "in which lowering blood pressure over hours or days, generally with oral antihypertensives, is preferred" [3]. Rest in a quiet room for 30 minutes, then measure again on the same arm, waiting 1–2 minutes between readings; if still above 180/110, see your family physician or the nearest emergency department the same day. The decision changes the moment headache, blurred vision, chest pain, shortness of breath, or altered consciousness appears — then call 112 immediately.
Can I give a sublingual capsule (Adalat / nifedipine) at home?
No. Short-acting sublingual nifedipine has long been removed from guideline-endorsed regimens for hypertensive crisis; it can drop blood pressure within minutes, reduce brain perfusion, and precipitate ischemic stroke or myocardial ischemia. The Turkish Society of Cardiology recommends "parenteral" — intravenous, in-hospital — lowering for hypertensive emergencies [3]. Instead of making a single-agent decision on scene, call 112 and hand over all of the patient's chronic-medication boxes to the ambulance crew.
Family physician, emergency department, or 112 — who should I call?
The decision tree runs on symptoms plus the number. (1) Blood pressure ≥180/120 mmHg with any warning symptom (chest pain, shortness of breath, severe headache, vision or speech change, altered consciousness, sudden weakness, vomiting) → call 112 immediately; if you prefer a specific private hospital, place a parallel Nova Ambulans call. (2) Number high (≥180/110), no symptoms → rest 30 minutes and remeasure; if still high, see a family physician or emergency department the same day in person. (3) Number 140–179/90–109 in a known chronic-hypertension patient → schedule a family-medicine visit for medication review. The 112 Command-and-Control Centre routes to the nearest hospital with the right intensive-care capacity when the call escalates.
My pregnant wife reads 150/95 and has a severe headache — what do we do?
The threshold is lower in pregnancy. After the 20th gestational week, readings ≥140/90 mmHg with headache, vision change, upper-abdominal pain, rapid edema, or reduced urine output define preeclampsia and sit on the doorstep of eclampsia (seizure). A reading of 150/95 is not "in the normal range" for a pregnant patient. Call 112 directly and report the gestational week. While waiting, place the patient in left-lateral decubitus, close the eyes, and keep the room quiet and dim. This picture can be fatal for the baby more than for the mother.
How do I know my home blood pressure monitor is accurate?
Choose an upper-arm digital cuff that appears on a clinical validation list; wrist cuffs are highly sensitive to deviation from heart level and are generally not recommended. Check your device's model at validatebp.org or on the Turkish Society of Hypertension and Renal Diseases recommended-devices list, and ask your family physician for a cross-comparison reading every six months. Before measuring: 5 minutes seated with back support, feet on the floor, no caffeine/smoking/exercise in the last 30 minutes, no talking during the reading.
My blood pressure is always high — am I still in danger?
Yes — even more so. The 2024 Boulestreau et al. review in the Journal of the American College of Cardiology identifies "non-adherence to the antihypertensive regimen" as the most common cause of malignant hypertension [8]. The body does not "get used to" high blood pressure; vascular-wall damage is silent, and kidney, retinal and cerebral white-matter micro-infarcts accumulate over years. Frequent readings above 180/120 indicate either an inadequate regimen or low adherence; review the regimen with a family physician or cardiologist. For what happens when uncontrolled hypertension drives a myocardial infarction, see our Heart Attack Symptoms and What to Do First guide.
Calling Nova Ambulans for a Hypertensive Emergency: When and Why
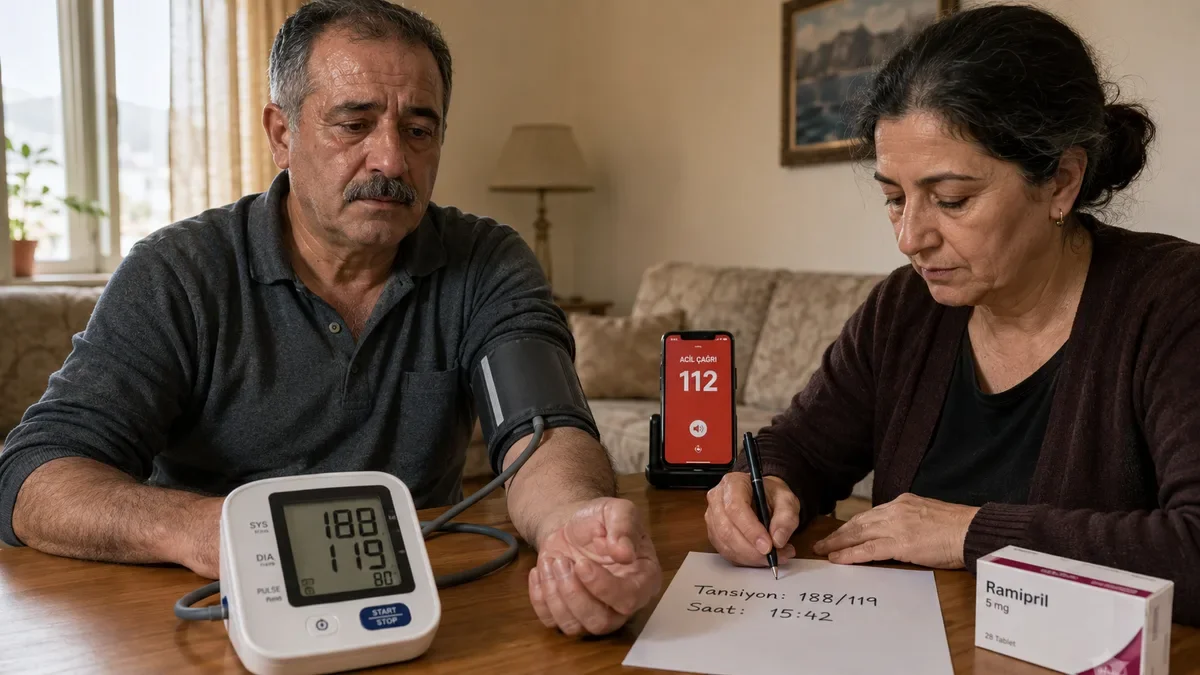
At 23:15 you find an elderly mother bedside with "188/115, my head is splitting, I can't see right" — three of the warning symptoms in one moment. Calling 112 and a parallel Nova Ambulans doctor-led ambulance brings two advantages: response-diversification (whichever crew is closer responds first) and hospital-choice flexibility (faster routing to the private hospital where your mother's cardiac records already live). A doctor-led ambulance for a hypertensive emergency means IV access opened en route, an initial IV antihypertensive available, and continuous ECG-and-rhythm oversight from an in-vehicle physician. The decision is unambiguous: symptoms + ≥180/120 mmHg = a medical emergency that needs minutes, not hours. Don't wait; note the number, gather the boxes, open the 112 call.
Related Posts
- Heart Attack Symptoms and What to Do First
- Stroke Symptoms and the FAST Test: A 4-Step Recognition Guide (2026)
- Winter Chest Pain and Shortness of Breath: 2025-2026 Season Emergency Decision
- Diabetes and Emergencies
- Home Care and Ambulance Support for Older Adults
- Difference Between 112 and a Private Ambulance
- How Long Does an Ambulance Take in Istanbul (2025)
Rapid Emergency Support
24/7 emergency ambulance service across Istanbul. Fast response, fully equipped team.
Average response time: 15 seconds
Related Articles
Asthma Attack First Aid: Step-by-Step Bystander Decisions and the 112 Chain
What a bystander does in the first five minutes of an adult asthma attack — the "5-minute rule" from the Turkish Ministry of Health's May 2025 First Aid Training Book, the mild/moderate/severe/life-threatening classification of the Global Initiative for Asthma (GINA) 2025 Summary Guide, correct metered-dose inhaler and spacer technique, differences for children, pregnant patients and the elderly, and Istanbul-specific triggers.
EducationWhen to Call an Ambulance for Seizures?
Learn in which symptoms you should call 112 or Nova Ambulans in seizure/convulsion situations seen in children and adults and the ambulance process.
EducationHome Medication Use: When to Call an Ambulance?
Learn when to call 112 or Nova Ambulans for dose errors, side effects, and sudden deterioration while using medication at home.
- Health Ministry: Between 2021-2025, 278,000 of those screened were diagnosed with hypertensionAnadolu Agency — based on Turkish Ministry of Health data ↗
- Death and Cause of Death Statistics 2024 ReleasedAnadolu Agency — based on Turkish Statistical Institute data ↗
- Turkish Society of Cardiology — Hypertensive Emergencies (National Hypertension Guideline)Turkish Society of Cardiology (TKD) ↗
- Turkish Society of Cardiology — National Hypertension Treatment Guideline (Classification)Turkish Society of Cardiology (TKD) ↗
- Turkish Hypertension Consensus Report 2025 (with seven contributing societies)Turkish Society of Hypertension and Renal Diseases (THBHD) ↗
- Hypertensive Crisis: When You Should Call 911 for High Blood PressureAmerican Heart Association ↗
- Hypertension Fact SheetWorld Health Organization ↗
- Malignant Hypertension: A Systemic Cardiovascular Disease (JACC Review)Journal of the American College of Cardiology — Boulestreau R, et al. ↗
- Prevalence, awareness, treatment, and control of hypertension in Turkey (the PatenT 2 study in 2012)Journal of Hypertension — Sengul S, et al. (PatenT2) ↗
Popular Ambulance Topic Clusters
You may also like
- Private ambulance pricing
- Istanbul private ambulance
- Intercity patient transport
- Doctor-accompanied ambulance
- Dialysis patient transport
- How intercity patient transport works
- Ambulance response time in Istanbul
- Home-to-hospital patient transport
- Modern ambulance equipment and team standards
- Heart attack symptoms and first response
This content is informational only and does not replace professional medical evaluation. In emergencies, call 112 or +90 216 339 00 39.